STRATEGIC FACILITIES PLANNING MODEL FOR PUBLIC PROPERTY - UK HEALTHCARE CASE STUDYTim BENNETT, United KingdomKey words: Facilities management; asset management; strategic facilities planning; National Health Service (UK). Public Sector property. AbstractThis work is posited as a work in progress and is a speculative paper based on a recent case study undertaken by the author. It describes various speculations concerning effective facilities planning and management of public healthcare sector property. The aim of the paper is to develop the conceptual framework within which activities should take place. To do this it draws upon a variety of types of study of asset management, and offers preliminary investigations on the validity of such facilities planning. The paper will consider the relationship between customer and business led strategies and how their different strategies affect facilities planning. A local healthcare economy within the UK National Health Service (NHS) will be used as a case study where the emphasis is now towards local 'mobile' patient care rather than hospital based 'static' care. The paper will aim to propose a prototype strategic model for healthcare property provision with the aim of testing and developing this framework at a later date for wider applications to aid the decision making process when considering facilities solutions to meet business needs and challenges. It is the proposal of this paper that facilities/asset strategies should be centred on business strategies and organisational aspirations rather than allowing the current assets, to dictate the direction of strategic business goals. The former approach allows the definition of a destination or destinations where as the latter approach provides and indication of the starting point and as a consequence the length of journey. A reversal of the focus will change the direction of the business strategy. This business focus rather than facility or asset focus allows strategies to be developed which once in place can then provide an informed platform for the more recognised facilities management models to come into play; cost in use, maintenance planning, space planning are just a few of the 'usual suspects'. The paper therefore proposes a two-staged approach. The need for this higher level of strategic planning outside the parameter of a physical asset is also highlighted by Then (1999) who identified three emerging themes requiring further research one being to link real estate/facilities decisions to corporate strategy. Then (1999) illustrates the critical interface that facilities management makes between strategic decisions and facilities provision issues - 'core business drivers' and 'affordability drivers'. The proposed model endeavours to encompass these two aspects by setting parameters for analysis, interpretation and dialogue so that asset planning can be taken out of the long grass and onto the fairway and formulate part of the business debate. The application to the NHS is merely a tool to attempt to facilitate the discussion and identify areas where clarity needs to be developed. It does however illustrate how past facilities planning driven by isolated decision processes has produced an imbalanced asset portfolio which has increased duplication in customer centred services, increased maintenance and operational costs and more importantly strategic business limitations when applied to an organisations aspirations within a changing marketplace. In relation to the NHS case study additional consideration could also be given to the additional services provided by local government such as social and unitary services which when added to the strategy overview may allow greater use of physical assets and develop customer service. The paper reflects early work in this area, and seeks to develop associations between the various factors mentioned. It does not purport to offer a definite solution, but to examine the context effective strategic facilities planning can offer to a model for further empirical study. 1. INTRODUCTIONThe move from the industrial age to the information age has meant that the skyline of an organisation's physical assets has changed dramatically. A recent consortium between General Motors and DaimlerChrysler where they have abandoned their stand-alone efforts has produced the world's largest virtual market, which will buy $240 billion worth of parts from tens of thousands of suppliers. Within days Toyota, Renault and Nissan all expressed interest in forging a similar approach (www.nua.ie 26 March 2000). This together with the growth of e-commerce, business to business (b2b) and business to customer (b2c) exchanges set out a new playing field for facilities planning. It is therefore clear that the starting point for strategic delivery is the business rather than the physical asset. Basing an organisations strategic goals on an extension of the past, can no longer be seen as a safe foundation on which to build business planning, and thus as a consequence asset planning. However, the business focus also presents a possible conflict where customer needs and wants cannot be fully met, as a business case cannot be made in terms of resources and or economic sustainability. The paper will attempt to discuss and test this issue. Tom Watson Jr., former President of IBM indicated (People Management 1999) that the value of his company was in its people. Remove the buildings and plant and keep the people and the information files and the organisation would be as strong as ever. This is not to say that the building as a facility is not important, it however does represent a small percentage of the true analysis of the meaning asset, more a 'direct' or 'tangible' asset. The key is to understand and identify the 'indirect' or 'intangible' assets, within the market perspective, which are the foundations to commercial success. The indirect assets of any organisation can be identified as 'Purchaser', 'Process' and 'People' assets. From this vantage point you can begin to develop strategies that provide facilities solutions that meet the business needs and challenges. The acid test is whether through the loss of one or more of the above could the organisation survive. When adding the direct asset to the equation, the supposition does not mean one should be at the expense of the other, rather that ownership and significance of the assets is not always equal. The balance between direct and indirect assets within the market context will be a key factor in strategic facilities planning. The emergence of 'dot.coms' has now added a new aspect to facilities planning with the realisation that virtual companies may not require space. The 'brick or click' factor may become the first question to ask in the boardroom or virtual boardroom when considering the need for physical assets. A recent example is the closure of the UK's Barclays Bank Plc premises in remote areas, which were seen not to be financially viable from the business perspective due to the growth in electronic banking. The organisation's customers/users however perceived the closures as a reduction in services and as a consequence detrimental to their needs. Interestingly the resultant closures helped the company's profit to show a healthy increase at the end of the financial year. This is an example of where customer and business aspirations differ. This does therefore raise the question as to who are the key determiners when considering facilities strategy, are they the customers/employees or is it the needs of the business. The two may be interlinked but different short and long term goals could be presented for each strategic focus. This friction is further demonstrated within the UK's National Health Service (NHS). It is the proposal of this paper that facilities/asset strategies should be centred on business strategies and organisational aspirations rather than current assets, to dictate the direction of strategic business goals. The former approach allows the definition of a destination or destinations where as the latter approach provides and indication of the starting point and as a consequence the length of journey. A reversal of the focus will change the direction of the business strategy. This business focus rather than facility or asset focus allows strategies to be developed which once in place can then provide an informed platform for the more recognised facilities management models to come into play; cost in use, maintenance planning, space planning are just a few of the 'usual suspects'. The paper therefore proposes a two-staged approach. The need for this higher level of strategic planning outside the parameter of a physical asset is also highlighted by Then (1999) who identified three emerging themes requiring further research one being to link real estate/facilities decisions to corporate strategy. It is this helicopter view, which will allow additional aspects such as the current and emerging business environment, which could include technology, work practices together with current corporate currency such as human resources and organisational culture to be considered as integral parts of the facilities planning process. This approach was highlighted by Kitchen (1997) who researched the range of NHS supporting services that fell under the responsibility of NHS Trust facilities managers and felt that this should go further. Further, Payne and Rees (1999) identified that there was a need to increase the portfolio of services to incorporate business focus areas as well. This paper therefore proposes a two-stage model for discussion, which attempts to provide this interchange, dialogue and overview. For the purposes of this paper the model will be applied to the UK's NHS with the intention of widening applications in due course. 2. UK - NATIONAL HEALTH SERVICE (NHS)Having recently celebrated its silver jubilee the NHS can be clearly identified as an organisation whose facilities strategy shows poor evidence of being considered at a national level or at a strategic level. Little of its operation currently benefits from a national perspective. It is unique in terms of its commercial counterparts, as governmental policy has played a large part in its creation, evolution and at times its downfall. Past strategic property planning within the NHS provided an impetus, which saw the publication in 1983 of a report entitled Under-used and surplus property in the NHS. This report set in motion a process, which led to the creation of a systematic approach to strategic planning and provided seven key stages as part of a framework for strategic decision-making. These centred around the development of strategic goals based on the interpretation of current assets rather than a strategy based on business aspirations, which in turn would then, determined the facilities strategy. The two approaches are different and would in the opinion of the author, lead to different outcomes. Currently procedural policy has moved away from 'internal markets' put in place under the UK Thatcher government of the early nineteen eighties. This produced a competitive environment of moat building and financial rivalry around local health provision. The only real benefit from this approach was that it created an understanding of health care value. This in turn enabled healthcare managers to understand the value of their assets. Current healthcare policy has now taken a different view with a three stage patient pathway with Primary, Secondary and Tertiary care with the initial stage of care being focused within the locality. Cases are then applied to the secondary care stage namely the acute hospitals. Rare health issues are then applied to regional or national areas or centres of excellent, which may only exist in a few locations within the country. This starts to provide a strategic framework for asset planning. The NHS however has not devised this framework on that basis, being more a political tool to improve the public's perception of the healthcare provision within the UK. This paper has undertaken to analysis this strategic approach to healthcare provision and superimposes a facility strategy onto the political framework that could become a template for future healthcare development within the NHS. A facility strategy by default! The very nature of the industry requires high level of employment and physical contact with customers. The research puts forward a two-pronged synopsis of what could be defined as the strategic approach to facility provision. SCOPE is an acronym for the customer and business led strategies:
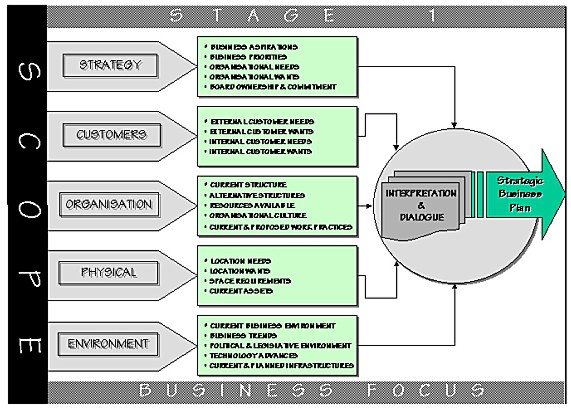
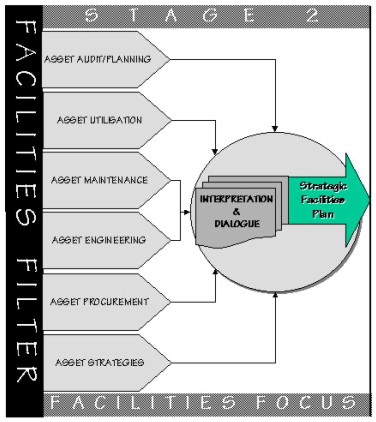
Figure 1. SCOPE Parameters The SCOPE model (Figure 2) allows a dual focus which in turn providers the arena to determine the key factors that will set the template for consideration for coalface facilities planning. The model was applied to current NHS provision within the Royal County of Berkshire in the UK. The application would be undertaken in two specific provision areas, namely local general practice facilities for a particular urban centre and secondly hospital services across the county as a whole. With this information 'Stage 1' of the SCOPE model would be applied to these two provision areas. From this information the research could be further developed to identify the practical steps needed to adapt and rationalise the current facilities to meet the revised business strategy. The planning process could then follow a process similar to that proposed by Then (1996) who identified Strategic Facilities Briefs and Service Level Briefs in the context of strategic and operational management. This would correspond to the second stage of the proposed model.
Figure 2. SCOPE Model
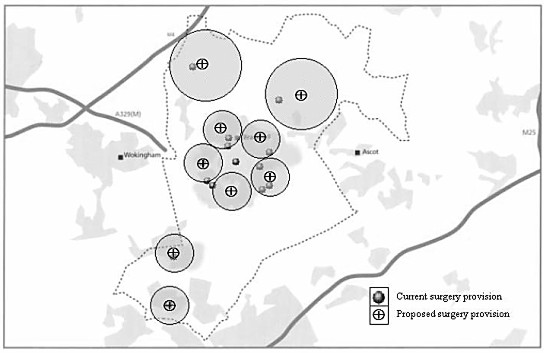
Figure 2. SCOPE Model 3. MODEL APPLICATIONResearch was undertaken within a specific urban area with a population of 101,000, which in the main was spread across three distinct areas with some outlying rural provision. The existing practices and hospitals were plotted (see figure 3 and 4 respectively) which identified a scatter approach rather than a planned collation to the population distribution. One reason for the current distribution could be accounted for by urban development unmatched by adequate healthcare funding together with inappropriate planning strategies by local authorities. The key component parts of the proposed model will now be applied in principle to the NHS case study:
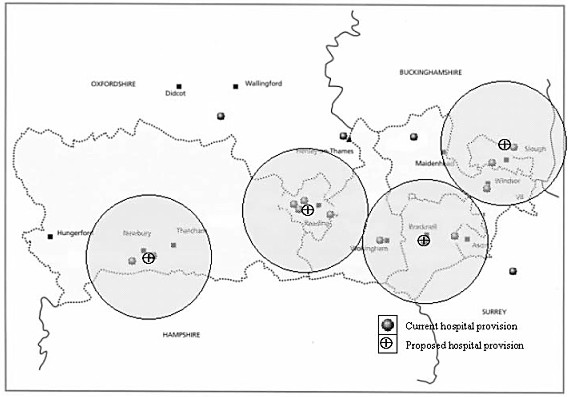
4. INTERPRETATION & DIALOGUEThe initial research undertaken did not show a clear strategy for implementation had been thought through at this time. The paper therefore sets out its own interpretation based on the analysis completed to date within the context of the proposed model. From the completion of the models Stage 1 a framework of healthcare provision can be proposed in an idealistic form which can provide clear parameters based on population density and distribution together with an understanding of customer wants and environment changes and forces. A survey was undertaken in January 2000 by the local Healthcare Forum, which comprises of local authority and local/county wide healthcare representatives. The aim of the study was to identify healthcare patterns within the local population of 101,000 to determine the users perception of their healthcare needs and wants. A questionnaire was sent to 43,500 homes of which 14,408 were returned, approximately one third. The questionnaire asked residents about their use of hospital based services and community based health services together with views on ease of travel and what services they would want to be provided more locally. The results were published (Bracknell Forest Health Panel Forum 2000) and showed that 55% of the respondents within the last twelve months visited the hospital within 15km of the town centre while 23.5% visited the hospital with a 25km radius compared with 21.5% who visited the hospital within 20km. Interestingly a large hospital within 22km was not identified as being visited. A large majority of the respondents (83.5%) identified that the nearest hospital (15km radius) was 'very' or 'quite' easy to access. One in eight (16.5%) travelled by public transport with the remainder using their own transport either as the driver or as a passenger. The survey identified that the greatest use of health services was the family doctor with 91.9% of respondents having used these service within the last twelve months. The survey further identified the healthcare 'wants' of the local community, which showed that nearly two-thirds stated they would like a more locally based Accident & Emergency (A&E) facility, one third mentioned the provision of a minor injuries unit and just under one third identified an out-patients clinic as being an important local service. The hospital based within 15km of the town center provides all the services identified by the respondents as being important. The survey data helps identifies the services that healthcare users perceive as important in terms of local provision together with an indication albeit by default of the acceptable travel distances for such services to provided within. Application of the Scope Model to this case study highlights the importance of the two-stage approach with the business focus leading the strategy. Stage one of the model incorporates the needs and views of 'purchasers' together with an analysis of physical assets and environment changes which in this case include Governmental moves to increase primary care with more and more services being centered around the family doctor. From this standpoint only can you then proceed to consider the strategy relating to the physical asset. A simple outcome of this case study when applied to the SCOPE Model could see the resultant facilities strategy. Currently there are 14 doctors practices serving the local healthcare economy under review, the research proposes a criteria that one practice should serve a population within a 4km radius with locations centralised within current or proposed transport infrastructures. By mapping locations based on this principle (see figure 3) it can be identified that the current provision of 14 practices can be reduced to 9. Areas of reduced population density would be served by practices with a greater circle of coverage say 8 - 16km mile radius. A 'walk-in centre' providing non-appointment services rather than being a dedicated doctors practice could serve the centre of the town. Simplistic although this process has been it has identified that purely setting a strategy based on facilities does not produce a cohesive business/customer led focus. The exact diameter of service coverage is not particularly relevant more that a framework has been applied which allows a qualitative analysis of service needs and strategic application based on the analysis interpreted under the SCOPE model. A similar exercise was applied to hospital provision applying a 15km radius based on the surveys findings that such a distance was acceptable in principle in locations with high population densities. Where densities are more wide spread e.g. for rural areas, catchment areas for hospital would have to be wider. This was plotted on the existing service provision map (see figure 4) and showed that current allocation of 17 hospitals could be reduced to 4. Naturally the original number of hospitals provided services for elderly and this may need to be added to local provision, as large travel distances may not be appropriate for such users. Areas with low population density could be served by mobile satellite services coming from the main hospitals linking with the increased services identified earlier that could be provided at the practice end allowing communication links with the hospitals reducing the needs for visits.
Figure 3. Doctor Surgeries: Existing & Proposed
Figure 4. Hospitals: Existing & Proposed 5. CONCLUSIONRees (1998) identified that the portfolio of facilities has increased over the previous two years, but highlighted the need for this to increase even further. Then (1999) illustrates the critical interface that facilities management makes between strategic decisions and facilities provision issues - 'core business drivers' and 'affordability drivers'. The proposed model endeavours to encompass these two aspects by setting parameters for analysis, interpretation and dialogue so that asset planning can be taken out of the long grass and onto the fairway and formulate part of the business debate. The application to the NHS is merely a tool to attempt to facilitate the discussion and identify areas where clarity needs to be developed. It does however illustrate how past facilities planning driven by isolated decision processes has produced an imbalanced asset portfolio which has increased duplication in customer centred services, increased maintenance and operational costs and more importantly strategic business limitations when applied to an organisations aspirations within a changing marketplace. In relation to the NHS case study additional consideration could also be given to the additional services provided by local government such as social and unitary services which when added to the strategy overview may allow greater use of physical assets and develop customer service. Further research will be undertaken to refine and develop the model by applying the principles in the first instance to other business sectors with the intention of producing a more structured decision making process for board level debate. The pilot research undoubtedly made some mistakes, but this was exactly the purpose of the primary study. The findings are of course, open to criticism from this nature and because of the small (arguable unrepresentative) sample. It has however provided both a framework for further work, and a model for immediate implementation to aid the learning and development process within the defined context of business strategy related asset planning. REFERENCES & FURTHER READINGAlexander, K. (Ed) 1996 Facilities management: theory and practice E & F N Spon Amaratunga, D. Baldry, D. & Sarshar M. 2000 Assessment of facilities management performance - what next? Facilities; 18:1/2 2000; pp. 66-75; ISSN: 0263-2772 Bracknell Forest Health Panel Forum. 2000 Improving health and Wellbeing Press release 6th March 2000; Bracknell Forest Town Council Bradley, S. & Woodling, G. 2000 Accommodating future business intelligence: new work-space and work-time challenges for management and design Facilities; 18: 3/4 2000; pp. 162-167 Davies C (Chairman) 1983 Under-used and surplus property in the NHS Enquiry report, HMSO Hosking, S. 1999 Healing the hospital environment: design, management and maintenance of healthcare E. & F N Spon Jones, O. 2000 Facility management: future opportunities, scope and impact Facilities; 18:3/4 2000; pp. 133-137; ISSN: 0263-2772 Kerns, F.1999 Strategic facility planning (SFP) Work Study; 48:5 1999; pp. 176-181 McGregor, W. 2000 The future of workspace management Facilities; 18:3/4 2000; pp. 138-143; ISSN: 0263-2772 Payne, T. & Rees, D. 1999 NHS facilities management: a prescription for change Facilities; 17:7/8 1999; pp. 217-221; ISSN: 0263-2772 Rees, D. 1997 The current state of facilities management in the UK National Health Service: an overview of management structures Facilities; 15:3/4 1997; pp. 62-65; ISSN: 0263-2772 Shiem-Shin Then, D. 1999 An integrated resource management view of facilities management Facilities; 17:12/13 1999; pp. 462-469; ISSN: 0263-2772 Smith, D. 1995 Changing roles and responsibilities in health-care facilities management Facilities; 13:1 1995; pp. 11-15; ISSN: 0263-2772 Spedding, A. (Ed.) 1994 CIOB Handbook of facilities management Longman Tompkins, J.A. (et al.) 1996 Facilities planning Wiley Wan Yeung Kam-Shim, M. 1999 Managing change: facilities management at the Pamela Youde Nethersole Eastern Hospital Facilities; 17:3/4 1999; pp. 86-90; ISSN: 0263-2772 Williams, B. & Associates 1998 Facilities Economics Building Economics Bureau Ltd Wrennall, W. 1999 Facilities design for an integrated structure Work Study; 48:4 1999; pp. 123-130 CONTACTTim P. Bennett 30 April 2001 This page is maintained by the FIG Office. Last revised on 15-03-16. |